IMPORTANT: Due to covid delays we are currently waiting on equipment from the US for this procedure so there is a waitlist.
Snoring
A medically proven Snoring Solution by trained and experienced doctors
Snore-Op is a minor surgery that requires topical and local anesthesia.
The procedure itself is painless, similar to the discomfort of having a small filling.
You can visit a Snore-Op trained doctor in all of the major New Zealand Regions.
High success rates backed up by medical research
Around 80% of our patients see a reduction with one treatment, and a further 10% respond to a second treatment. Find out why Snore-op is such a successful cure for snoring.

Quick and unobtrusive
Snore-Op is a minor surgery that is done in the doctor’s office and the entire process only takes 45 minutes . Watch the video to see how easy it is! You can also read more about the Snore-op procedure
Experienced Doctors
Dr Neil Hutchison and Dr Andrew Murley have performed over 3,000 Snore-Op procedures since they began developing the treatment in 1997. That’s a lot more happy spouses! Meet the snoring experts.
Affordable
Treatment costs $945 and includes the discussion, check for suitability, the minor surgery, and non-operative followups.
General information
Snoring
This is a very disruptive and common problem. It is generally made by vibration of surfaces together in the upper airway. Most snoring noise emanates from the soft palate, and is louder when the mouth is open. Other sites contributing may be the back of the tongue and the nose, and sometimes structures in the lower throat. Between 30 and 40% of the population snores, and it seems to be more common in men. As one gets older, snoring frequency and loudness increase owing to the reducing levels of “elastin” in aging tissues. Weight gain, smoking, alcohol, sedatives, and back sleeping often worsen snoring. Some other factors are not easily solved such as small lower jaw, and some have large tonsils which may need to be removed to reduce the problem. Bad snorers can wake very tired, or have daytime sleepiness. Snoring has also been implicated as an aggravating factor in other medical problems such as hypertension and depression. Fixing snoring does not necessarily solve these problems.
Sleep Apnoea
This is the cessation of breathing for a variable length of time in sleep. This is caused by obstruction to the airway with the tongue, and results in falling oxygen levels. This is often associated with a number of health problems, and can be diagnosed with “Sleep Study”. This condition is often the source of most concern to the partner, and may occur in as many as 10% of adults.
Options for the snorer
the options for the snorer are quite varied, and really depend on where the snoring originates. This is determined by the examination of a doctor experienced in this field. Doctors trained in the “Snore-Op” method have had extra training in this examination and technique. Most people who present to the doctor have tried a range of treatments with limited success. Most methods have benefit for some patients and range from throat and nose sprays, nasal splints, jaw advancements splints, to minor and major surgical corrections.
The Snore-Op
The Radio frequency Tissue Volume Reduction technique (e.g. “Snore-Op”) is amongst the most likely to succeed (around 80% of our patients have a reduction with one treatment, and a further 10% respond to a second treatment). It is a minor operation requiring only local anaesthesia, and done in the doctor’s office. It is very like a trip to the dentist, where local anaesthetic is used to numb the palate, and two small areas of the soft palate are treated painlessly. The snoring gets worse for two or three nights, then lessens progressively over about 2 months. Most notice initial improvements from about 14 to 21 days postoperatively. The effectiveness and longevity of these results varies in individuals. A patient who reduces his snoring to less than “3” on the snoring scale below is likely to have a result lasting 3 to 5-plus years in our experience. Other treatment options will also “wear off” with increasing age and weight. It is a very simple matter to repeat this treatment, and it is very cost-effective. Much of this method was pioneered and developed by New Zealand doctors, and is now used world-wide.
In a survey of fifty patients, they were asked to rate the pain they felt after the anaesthetic wore off. They rated the pain on average 2/10, ranging from zero to four. Only a quarter of them felt they needed mild analgesia. However, some choose to take two panadeine prior to the operation to cover the possibility of pain when the local wears off ninety minutes later. Anti-inflammatories and aspirin-like drugs are not recommended.
People who have had the major surgical operations (UPPP and LAUP) can have a “Snore-Op” to re-tighten their palates. This has been very effective in certain cases.
The post-operative phase
It is recommended that cool fluids and ice are used to reduce inflammation the first evening. Difflam anti-inflammatory oral spray can be a help in some cases. Non-aspirin-like analgesics are recommended for the people who do wish to take tablets. The swelling that often occurs of the Uvula (dangling from the back of the palate) is reduced by sleeping on a slope of 30 to 45 degrees for one to three nights, and in worst cases, gargling with a strong salt solution. Eating and drinking present no major problems. Speech can be temporarily affected, lasting at the most two to three days.
You will be given a “Post-operative Trouble Shooting Sheet”, with the contact number of your doctor, should you need to call him after hours. Any fever or increasing pain should be notified to your doctor.
Follow-up is recommended at between three and seven days, and another visit eight weeks post-operatively. A further treatment can be carried out at the eight week visit when the improvement reaches a plateau if there is insufficient response.
Cautions
- People with cardiac pacemakers should not have this procedure without consulting their cardiologist.
- Snoring usually gets worse for a few nights, but this soon passes.
- Very rarely, a patient has an allergy to the local anaesthetic. If you have not had a reaction to a dental injection, there should be no problem.
- Also very rare is a perforation of the palate, which heals quickly and well. This is avoided by effecting burns mainly to the thickest part of the palate.
- Those with heart valve disease, or artificial heart valves, or artificial joints should mention this in the pre-operative discussion with your operating doctor. These present a minimal risk, but should be considered.
- Those who are known to have Hepatitis B or C, or those who may be HIV positive should also inform their doctor in confidence of their condition.
Additional Surgery
Some people may need a similar procedure with radio frequency surgery performed on the turbinate tissues of the nose. This option will be assessed at the initial visit, and is usually not required. Turbinate surgery, which is usually totally painless after the local anaesthetic, is done when the blocked nose is considered part of the problem. Some might also require the uvula shortened where this is large and thought to be problematic. These minor operations can be carried out where necessary with the palate procedure.
Anatomy in Snoring
Tongue: Attached mainly to the jaw bone, this heavy organ can drop backwards and obstruct the airway. This mainly occurs with back sleeping, and is the main explanation for Obstructive Sleep Apnoea. Although the breathing appears to stop in this condition, the efforts to breathe continue until it suddenly clears. This is often a noisy event, sometimes even waking the patient. To test if the snoring involves the tongue, one can simply protract (protrude) the jaw and see if the noise ceases. This is also a good test to see if a mouthguard jaw advancement splint is likely to help snoring noise. In our experience, the tongue is not a common source of the disturbing snoring noise. It is after all much more difficult to make half a pound of meat (the tongue) shake than the thin membrane that we call the soft palate!
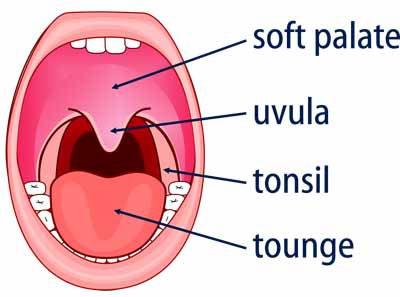
Soft Palate: The usual source of the disturbing noise of regular snoring. As one gets older, the elastin in the tissues (ie the rubberyness) reduces, and what stretches stays stretched. This is why we get wrinkles in the skin more as we get older. The same applies to the palate, which becomes permanently overstretched with all the flapping, and the snoring thus gets worse with aging. The palate gives rise to the familiar rattle of snoring sometimes referred to as “Sawing wood” as it is noisy and regular. The rattle occurs as the soft palate vibrates against the back of the naso-pharynx much as two pieces of paper vibrate when one blows between them. As the gap between the sheets increases, the rattle decreases. The concave soft palate will come forward when it shrinks in response to a “Snore-Op”. This brings the two surfaces further apart, and they will stop vibrating is the gap between them is sufficient.
Turbinate’s: These are the heat, filtering and moisturising wrinkles on the outer wall of the nose cavity. When enlarged, these can block the nose. This is a cause of mouth breathing often seen in snorers. In some, the turbinates require shrinking to allow more air up the nose. This in turn allows one to sleep with the mouth closed, which reduces the loudness of the snoring rattle. “Snore-Op” can be used to reduce the size of the turbinates as a small office procedure, done even at the same time as the palate operation. Alternatively, a much larger operation requiring hospitalisation can be done to clear the nose.
Uvula: It is not clear what the Uvula does, and if large enough, or wide enough, it may vibrate like the soft palate. One of the beauties of “Snore-Op” is that the procedure tends to reduce the size of the uvula.
The Snoring Scale is useful for measure the loudness and effects (disturbance factor) of your snoring.
- No snoring at all
- Non-disruptive slight snoring sometimes
- Non-disruptive slight snoring about half the time
- Non-disruptive snoring most nights
- Disrupts partner sometimes
- Disrupts partner about half the nights
- Disrupts partner every night
- Disrupts others through shut doors some nights
- Disrupts others about half the nights of the week
- Disrupts others every night in other rooms
- Partner sleeps in another room often
For a more accurate measurement, your partner’s opinion is required.
Your Results
0-3 Your snoring is having minimal impact.
3-10 Your snoring is disturbing other people.
If your snoring has become disruptive (higher than 3) snore-op could be beneficial
General information:
Snoring is a very disruptive and common problem. It is generally made by vibration of surfaces together in the upper airway. Most snoring noise emanates from the soft palate, and is louder when the mouth is open. Other sites contributing may be the back of the tongue and the nose, and sometimes structures in the lower throat. Between 30 and 40% of the population snores, and it seems to be more common in men. As one gets older, snoring frequency and loudness increase owing to the reducing levels of “elastin” in aging tissues. Weight gain, smoking, alcohol, sedatives, and back sleeping often worsen snoring. Some other factors are not easily solved such as small lower jaw, and some have large tonsils which may need to be removed to reduce the problem. Bad snorers can wake very tired, or have daytime sleepiness. Snoring has also been implicated as an aggravating factor in other medical problems such as hypertension and depression. Fixing snoring does not necessarily solve these problems.
Sleep Apnoea is the cessation of breathing for a variable length of time in sleep. This is caused by obstruction to the airway with the tongue, and results in falling oxygen levels. This is often associated with a number of health problems, and can be diagnosed with “Sleep Study”. This condition is often the source of most concern to the partner, and may occur in as many as 10% of adults.
Options for the snorer are quite varied, and really depend on where the snoring originates. This is determined by the examination of a doctor experienced in this field. Doctors trained in the “Snore-Op” method have had extra training in this examination and technique. Most people who present to the doctor have tried a range of treatments with limited success. Most methods have benefit for some patients and range from throat and nose sprays, nasal splints, jaw advancements splints, to minor and major surgical corrections.
The Snore-Op: The Radiofrequency Tissue Volume Reduction technique (eg “Snore-Op”) is amongst the most likely to succeed (around 80% of our patients have a reduction with one treatment, and a further 10% respond to a second treatment). It is a minor operation requiring only local anaesthesia, and done in the doctor’s office. It is very like a trip to the dentist, where local ™ anaesthetic is used to numb the palate, and two small areas of the soft palate are treated painlessly. The snoring gets worse for two or three nights, then lessens progressively over about 2 months. Most notice initial improvements from about 14 to 21 days postoperatively. The effectiveness and longevity of these results varies in individuals. A patient who reduces his snoring to less than “3” on the snoring scale below is likely to have a result lasting 3 to 5-plus years in our experience. Other treatment options will also “wear off” with increasing age and weight. It is a very simple matter to repeat this treatment, and it is very cost-effective. Much of this method was pioneered and developed by New Zealand doctors, and is now used world-wide.
In a survey of fifty patients, they were asked to rate the pain they felt after the anaesthetic wore off. They rated the pain on average 2/10, ranging from zero to four. Only a quarter of them felt they needed mild analgesia. However, some choose to take two panadeine prior to the operation to cover the possibility of pain when the local wears off ninety minutes later. Antiinflammatories and aspirin-like drugs are not recommended. People who have had the major surgical operations (UPPP and LAUP) can have a “Snore-Op” to re-tighten their palates. This has been very effective in certain cases.
The post-operative phase: It is recommended that cool fluids and ice are used to reduce inflammation the first evening. Difflam anti-inflammatory oral spray can be a help in some cases. Non-aspirin-like analgesics are recommended for the people who do wish to take tablets. The swelling that often occurs of the Uvula (dangling from the back of the palate) is reduced by sleeping on a slope of 30 to 45 degrees for one to three nights, and in worst cases, gargling with a strong salt solution. Eating and drinking present no major problems. Speech can be temporarily affected, lasting at the most two to three days.
You will be given a “Post-operative Trouble Shooting Sheet”, with the contact number of your doctor, should you need to call him after hours. Any fever or increasing pain should be notified to your doctor. Follow-up is recommended at between three and seven days, and another visit eight weeks post-operatively. A further treatment can be carried out at the eight week visit when the improvement reaches a plateau if there is insufficient response.
Cautions:
People with cardiac pacemakers should not have this procedure without consulting their cardiologist.
Snoring usually gets worse for a few nights, but this soon passes.
Very rarely, a patient has an allergy to the local anaesthetic. If you have not had a reaction to a dental injection, there should be no problem.
Also very rare is a perforation of the palate, which heals quickly and well. This is avoided by effecting burns mainly to the thickest part of the palate.
Those with heart valve disease, or artificial heart valves, or artificial joints should mention this in the pre-operative discussion with your operating doctor.
These present a minimal risk, but should be considered. Those who are known to have Hepatitis B or C, or those who may be HIV positive should also inform their doctor in confidence of their condition.
Additional Surgery:
Some people may need a similar procedure with radiofrequency surgery performed on the turbinate tissues of the nose. This option will be assessed at the initial visit, and is usually not required. Turbinate surgery, which is usually totally painless after the local anaesthetic, is done when the blocked nose is considered part of the problem. Some might also require the uvula shortened where this is large and thought to be problematic. These minor operations can be carried out where necessary with the palate procedure.